We Need To Talk About Long COVID

Death is not the only metric that matters. We need to talk about the lives lost to COVID, even if people survive. We need to talk about Long COVID. As Dr. Akiko Iwasaki says, “millions of people are currently suffering from devastating impact of long COVID.” This entire piece is based on a lecture she gave to the FNIH.
We have got to this dreary slog because of bad choices certain people made, and I want to talk about that first. Instead of eliminating this disease, Western countries came up with the craven concept of ‘living with the disease’. This is why individuals are literally living with the disease for years now. This is no way to live.
We have failed Long COVID patients by getting them into this situation, and we fail them even further by not taking Long COVID seriously. These people have been patient long enough. They’ve been suffering for over a year now. The least we can do is listen.
Long Disease Is A Thing
Part of the problem is that we don’t give significant fucks about chronic illness at all. Even doctors misdiagnose or just don’t diagnose chronic problems, especially vague ones like chronic fatigue. The general population equates fatigue with ‘just being tired’ and the answer to to just shut up and rest. But when you can’t stand in the shower for months, something is seriously wrong. As one doctor reports;
“One patient told me: ‘Dr. Ely, I wish that my hand was cut off so that people could see that something was wrong with me. But as it is when they look at me, they think I’m fine. And I’m completely diseased and burdened by these problems of long COVID, and everybody thinks I’m OK, and it makes it worse for me,’” Ely said.
The response to lots of chronic disease is often just wait, lose weight, or some variant of ‘just go away’. But the disease doesn’t go away. That’s literally the fucking problem. We’re just telling suffering people to go away.
One part of the problem is that if a disease is unknown or uncommon we tend to think it’s unreal. The idea of a COVID infection that doesn’t go away is so unusual that it fits into the same category. We’re not used to people having Long Cold or Long Flu, but one of the points Iwasaki makes is that we have known about other long infections for a long time.
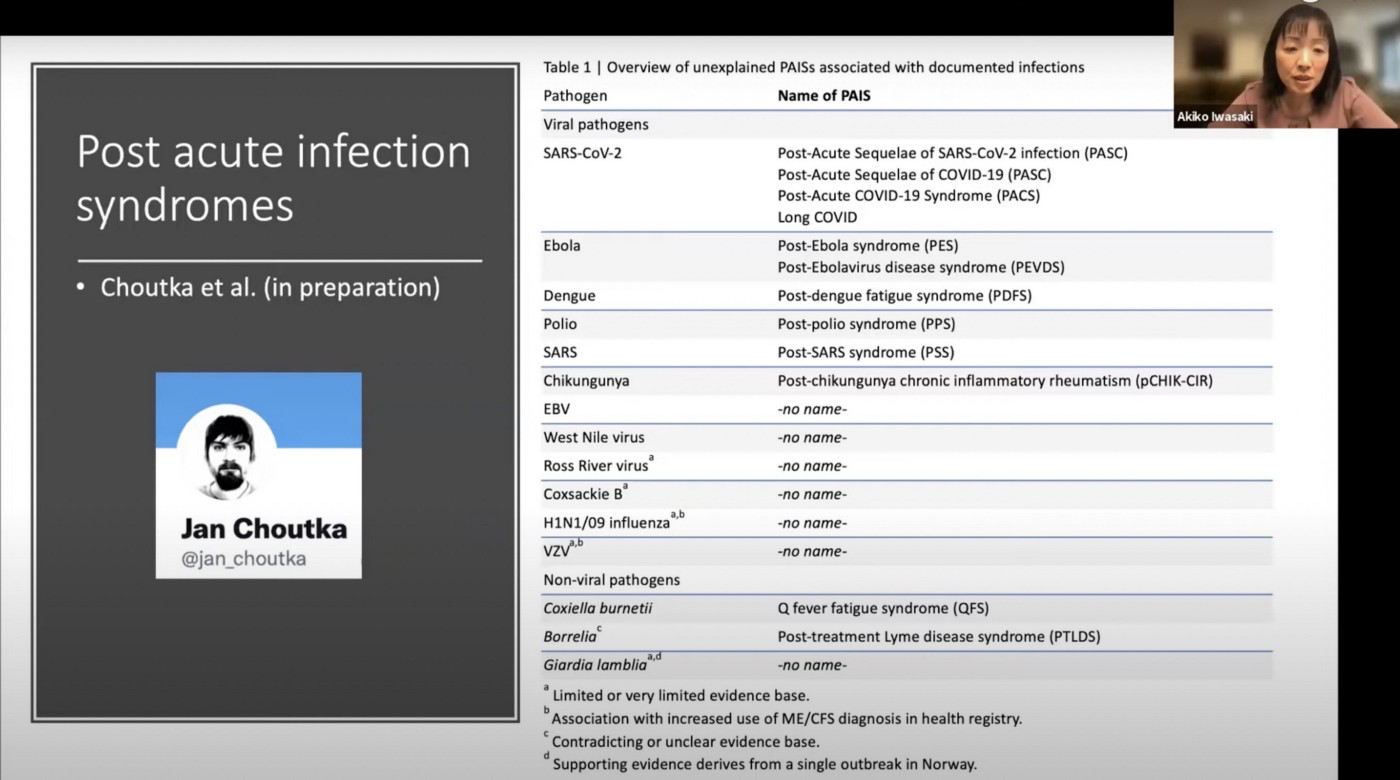
Here’s a list. I’ve had some form of post-dengue for months and it sucked. The trouble is that these are mostly neglected tropical diseases within the neglected category of chronic illness, making the whole category neglected AF. This is unfortunate because, as mentioned, the symptoms suck.
Long COVID Is A Thing
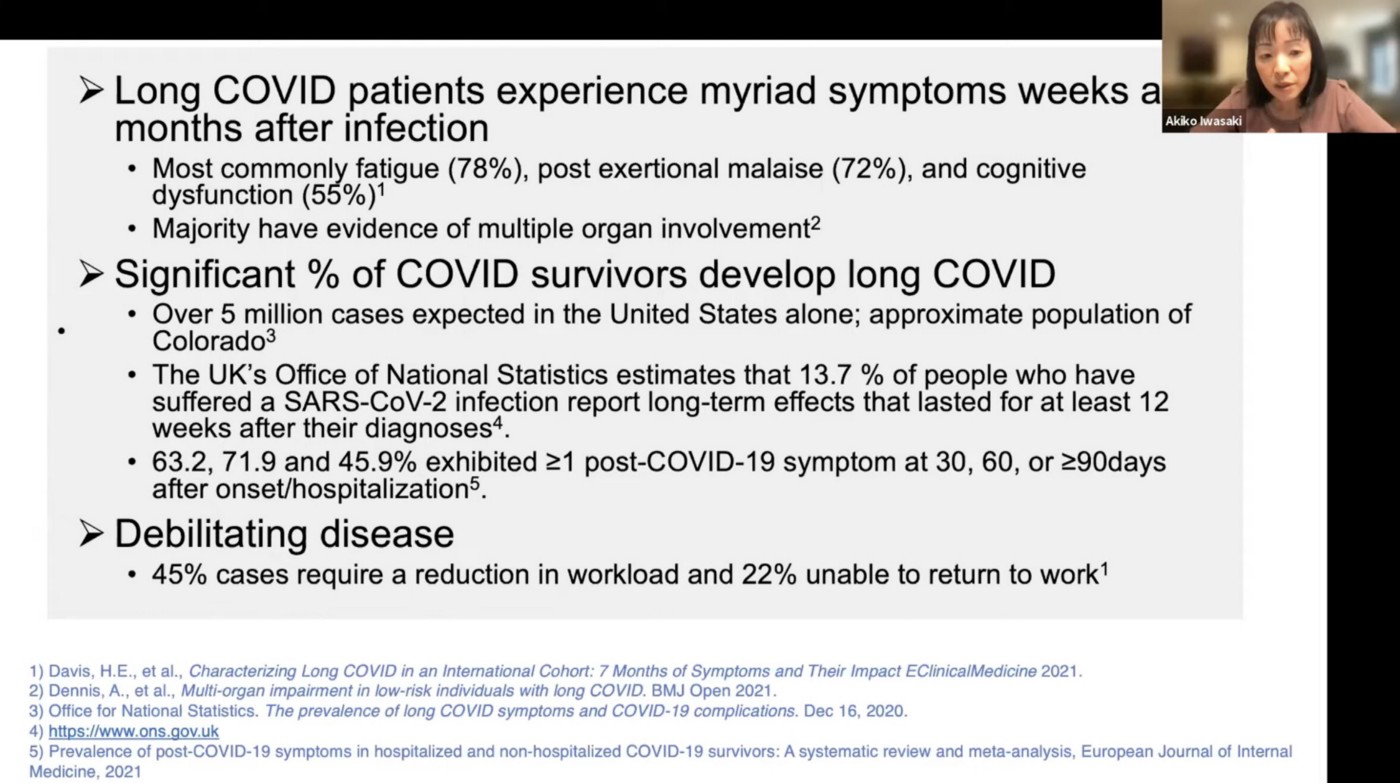
Long COVID is thus a thing within this category of things. Given that COVID is everywhere, this is no longer a neglected tropical problem. It’s a neglected global problem and it’s staggering in scale. Clinical definitions of Long COVID vary and every case is certainly not reported. Iwasaki calls it a ‘significant %’ which is scientist for *screaming*.
The political petri dishes of the US and UK report high numbers which are certainly a floor, not a ceiling. The equivalent of the entire state of Colorado (5 million) has Long COVID in the US and at least 14% of all reported cases in the UK. These are numbers but I encourage you not to think about it this way. That thinking is part of the problem. Zero should have been the goal from the beginning. Elimination of COVID, as China did. Instead we’re here, gambling and bargaining with human lives. It’s sick.
Long COVID Sucks
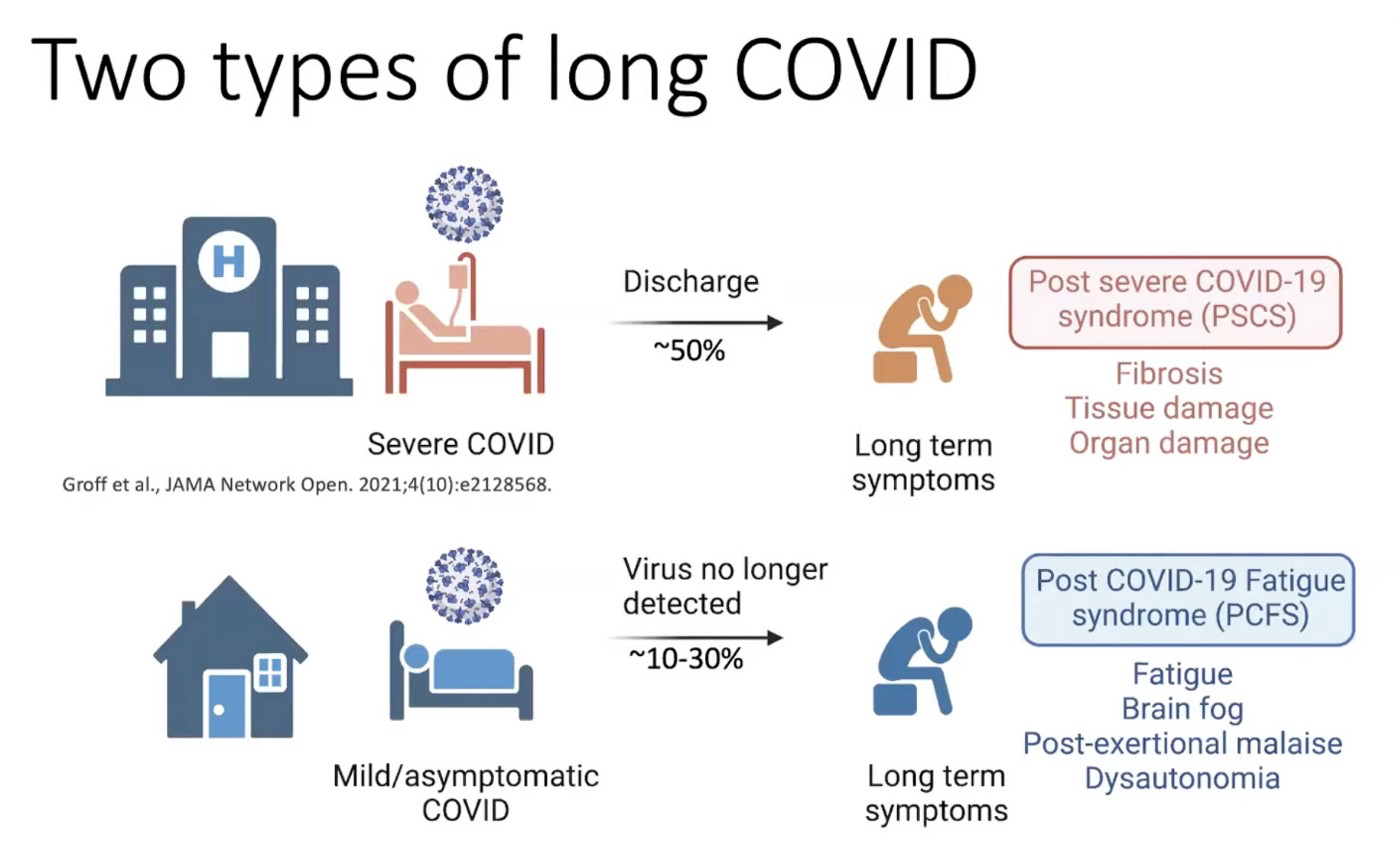
So don’t think about these problems in a population. Think of them in you. Of people who went through the horrorshow of severe COVID, 50–70% of them get reruns for months. And these symptoms are fucked up. Fibrosis, tissue damage, organ damage. Major hull damage, Captain!
Of people who get ‘mild’ COVID, roughly 10–30% get ongoing fuckery of the body, brain, and mind. If you consider these symptoms ‘mild’ try having them yourself. I had fatigue and ‘brain-fog’ from a dengue-ish viral infection and it was fucking debilitating. I wouldn’t wish that on anyone.
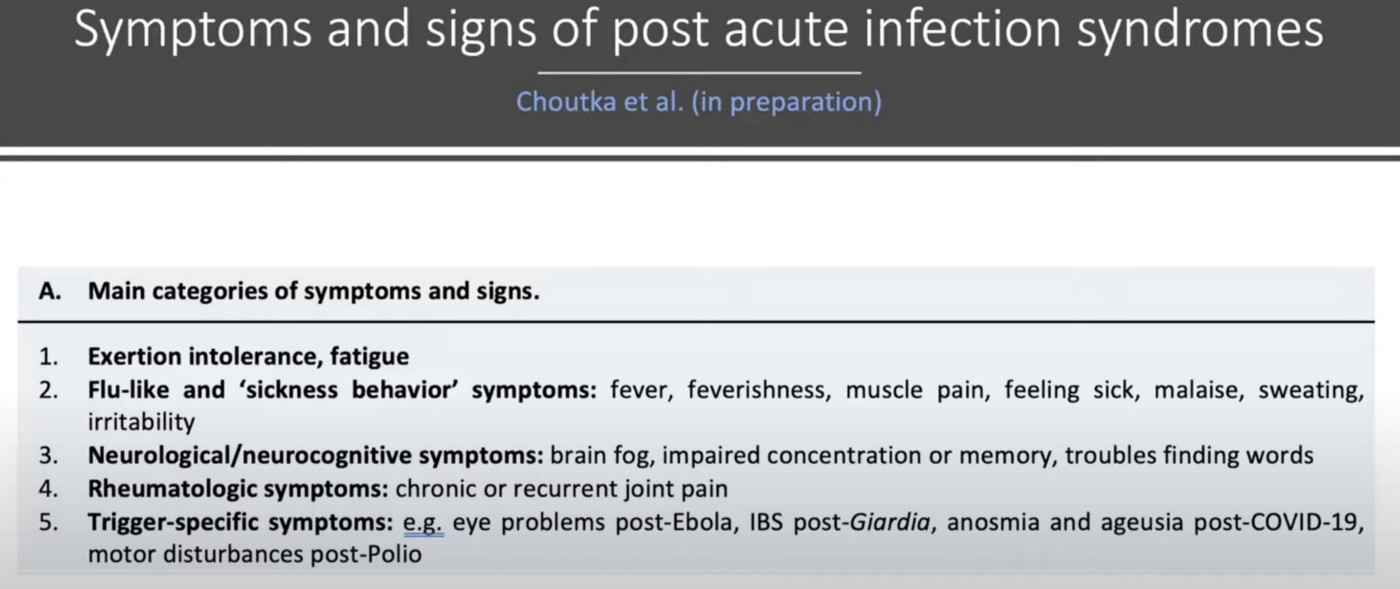
What happens with Long COVID is full body fuckery. We’re talking about multiple organ systems.
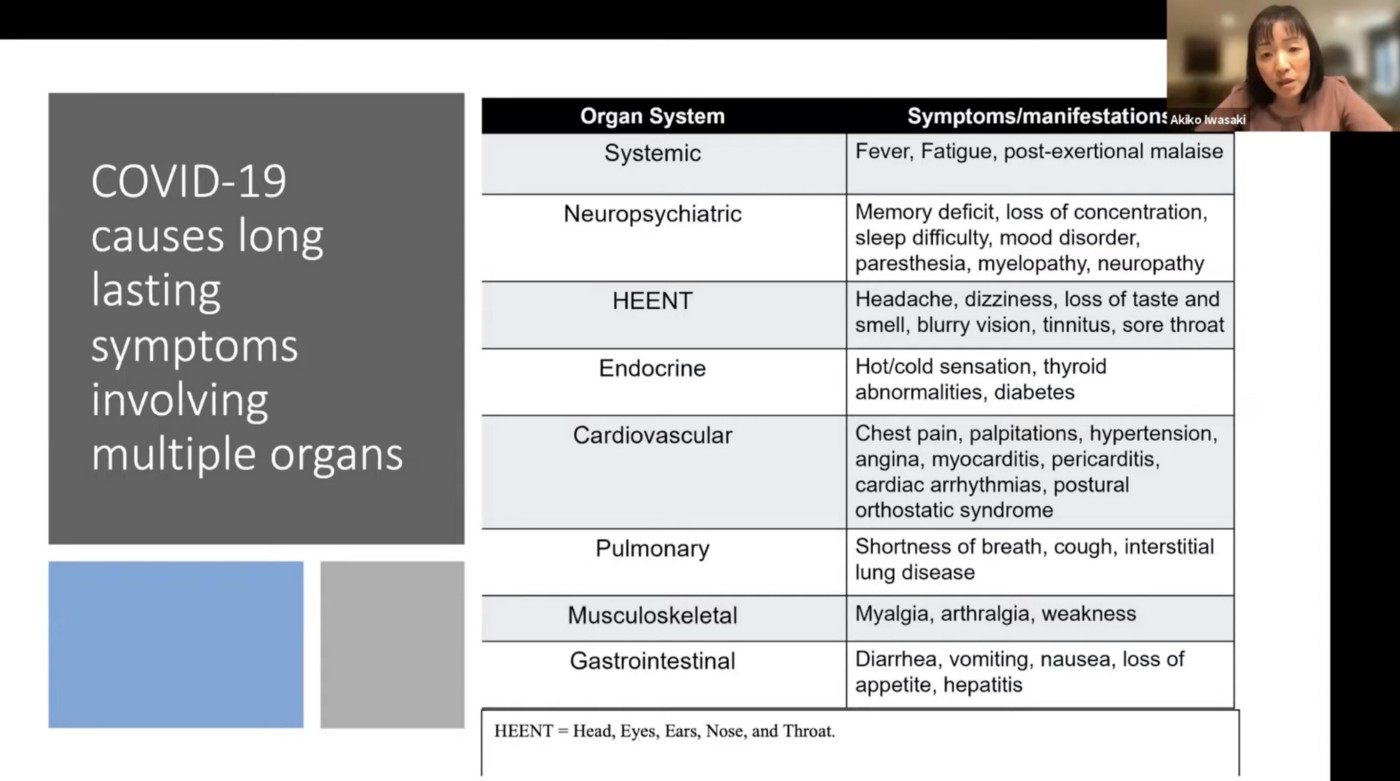
Of these effects, the most common is fatigue (a general term encompassing a unique misery) followed by the inability to exert yourself, which can mean going up the stairs, showering, and certainly exercising. For anyone with children or even just a life, this is hard.
Another highly common symptom is the also easy to write-off ‘brain fog’. We might joke about this in normal life, but in clinical terms it means the most important organ in the human body is not working. As survivor Pennysays, “brain fog sucks dude ive had it since ive gotten covid and its even worse these days, my mind is constantly in a haze and I forget how to do the simplest things, its scary.”
The term ‘fog’ really doesn’t to it justice, as survivor Michael A. Osborne says:
Again, don’t look at this as numbers. Look at this as people suffering from an entirely prevantable disease. Look at this as long-term consequences that we don’t know the end of. If this was your life you would take it very seriously. We need to take this seriously in others.
It Seems Worse For Women
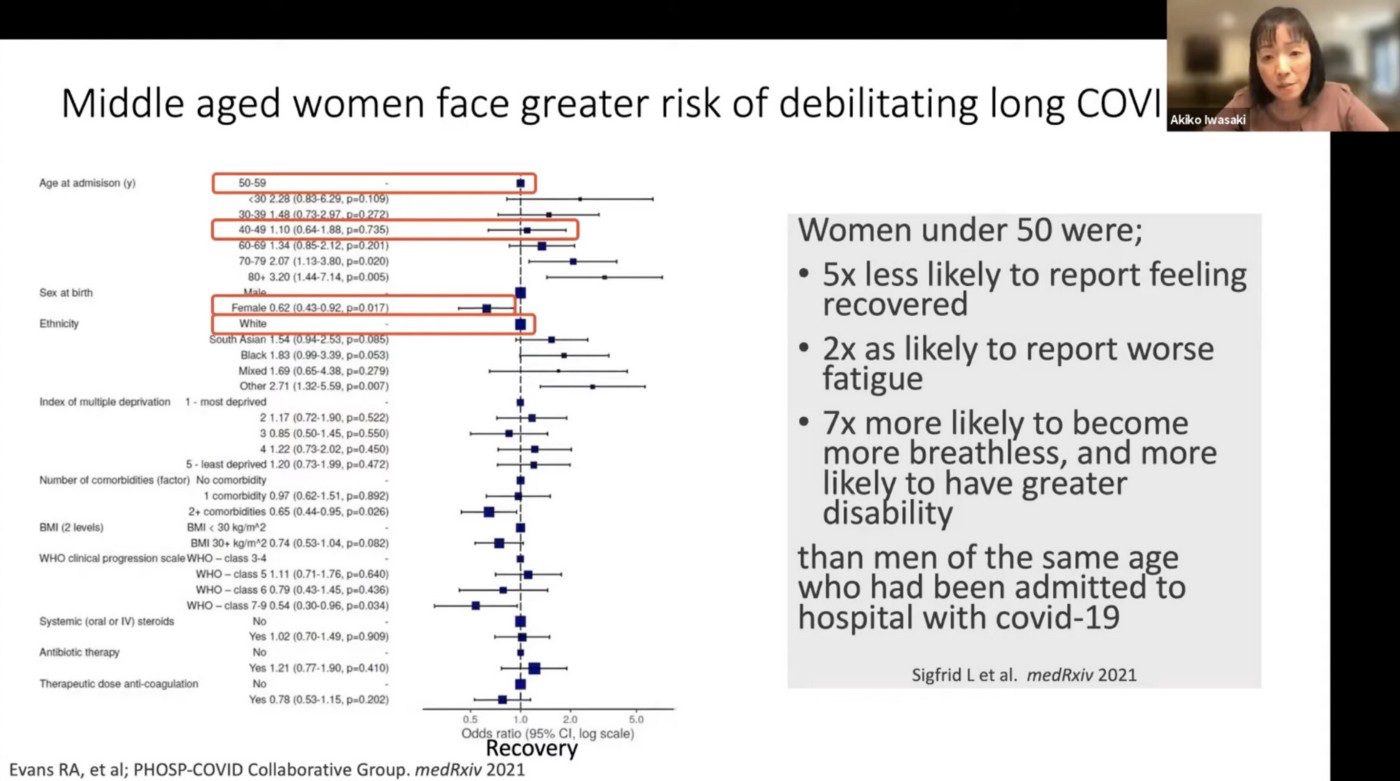
Like life in general, Long COVID seems harder on women. In a batch of disparate studies, women were 7X more likely to become more breathless than men. Given that women’s pain is often ignored by doctors, the numbers are likely much worse.
Long COVID May Mean Literally Still Having COVID
Iwasaki says “It’s potentially possible for these people to have failed to clear the primary infection, that may be leading to some other long-term consequences.”This is just one of the possible mechanisms of Long COVID but I mention it first because it’s the most fucked up.
It means that COVID may be hiding out, undetectable (ie, not where we swab), providing human reservoirs for further mutation, misery, and strife. As she says, the somewhat rare loss of smell (anosmia) and diarrhea associated with COVID may mean that the virus is hiding out there (as opposed to the lungs). As Iwasaki said:
We know that the long-haulers have no longer detectable levels in their [nose] or saliva. However, it is possible that there are remnants of virus in various different tissues. If that were to happen, there may be chronic inflammation that result in long-term symptoms.
That is, the fact that people are having problems in all these organs may mean that COVID is lurking in all these organs. There’s evidence for this in intestinal biopsies which found that, after three months, 5/14 patients had positive staining (ie, you could see virus) and 3/14 had PCR positive tests (ie, you could find COVID in this normally untested part of the body). Note that this is out of 14 people in a selective sample, you can’t extrapolate this to any population per se.
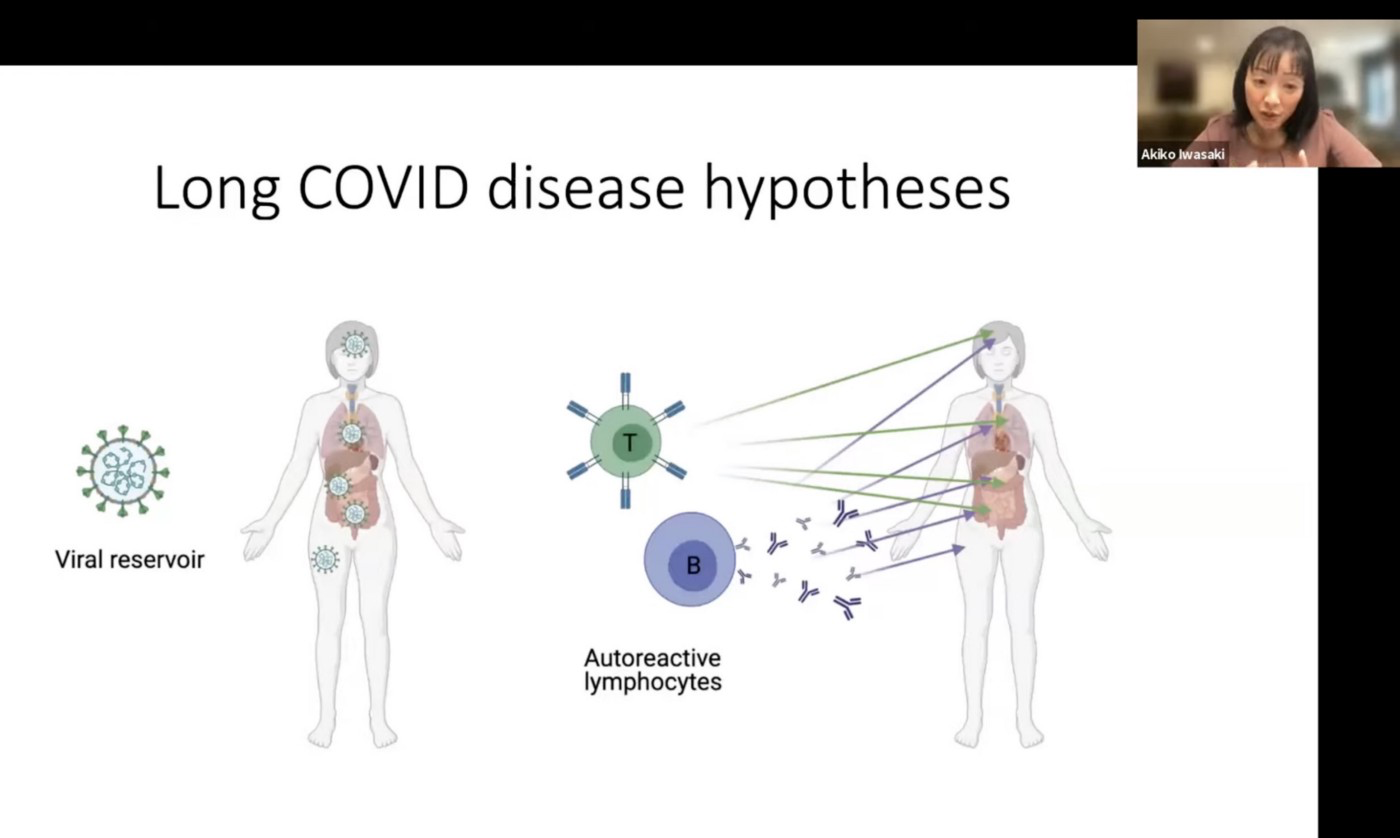
Iwasaki called this the possibility of “having a viral reservoir or viral ghost,”in picturesque and terrifying terms. Carrying virus around like this is literally having bugs crawling underneath your skin. It’s not fun. It’s also completely fucked in public health terms because it would mean the virus is just chilling and mutating into God knows what form.
Long COVID May Fuck Up Your Immune System
My immune system responds to peanut as if it’s World War III. I have a ‘mild’ allergy which is actually miserable and gives you a sense of autoimmune disease. The problem is not necessarily the foreign particle (peanut doesn’t actually do anything to me) but your body’s reaction to it. It’s very scorched earth. This seems to be part of the problem with Long COVID.
Your body may eliminate COVID, but like America after World War II, it never draws down its troops. And these autoreactive lymphocytes, etc continue attacking healthy tissue.
Research with Aaron Ring et al ‘probed for the presence of autoantibodies’ and found them. They’re still following up with these patients a year later. One recent study found certain autoantibodies in all patients with long-term symptoms (again, can’t be generalized to a population).
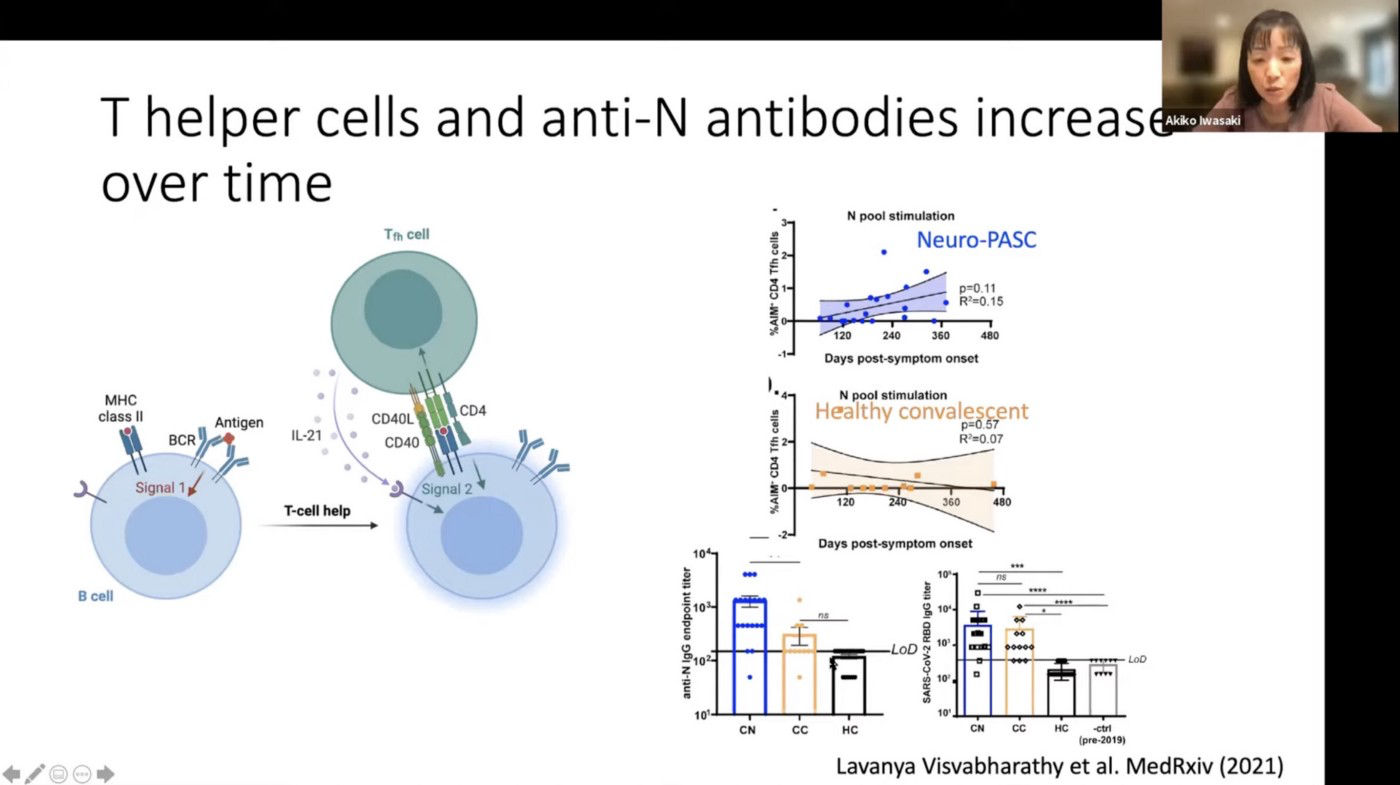
In another study, patients with Long COVID (called Neuro-PASC above) have continuously elevated levels of T-cells whereas the defenses of healthy people draw down over time.
Again and again, you can’t generalize from any of these studies but it seems obvious that some shit is going on. Long COVID certainly isn’t in peoples’ heads, we can measure it in their bodies. There’s evidence for both these hypotheses, and it may in fact be combinations of the two (or more). As Iwasaki says, “this is all hand-waving, as I’m literally hand-waving. We don’t know. Right now I’m still completely open to all hypotheses of Long COVID.”
We don’t know the exact pathology of Long COVID, but we can reasonably say that it’s pathological.
Long COVID Is Long
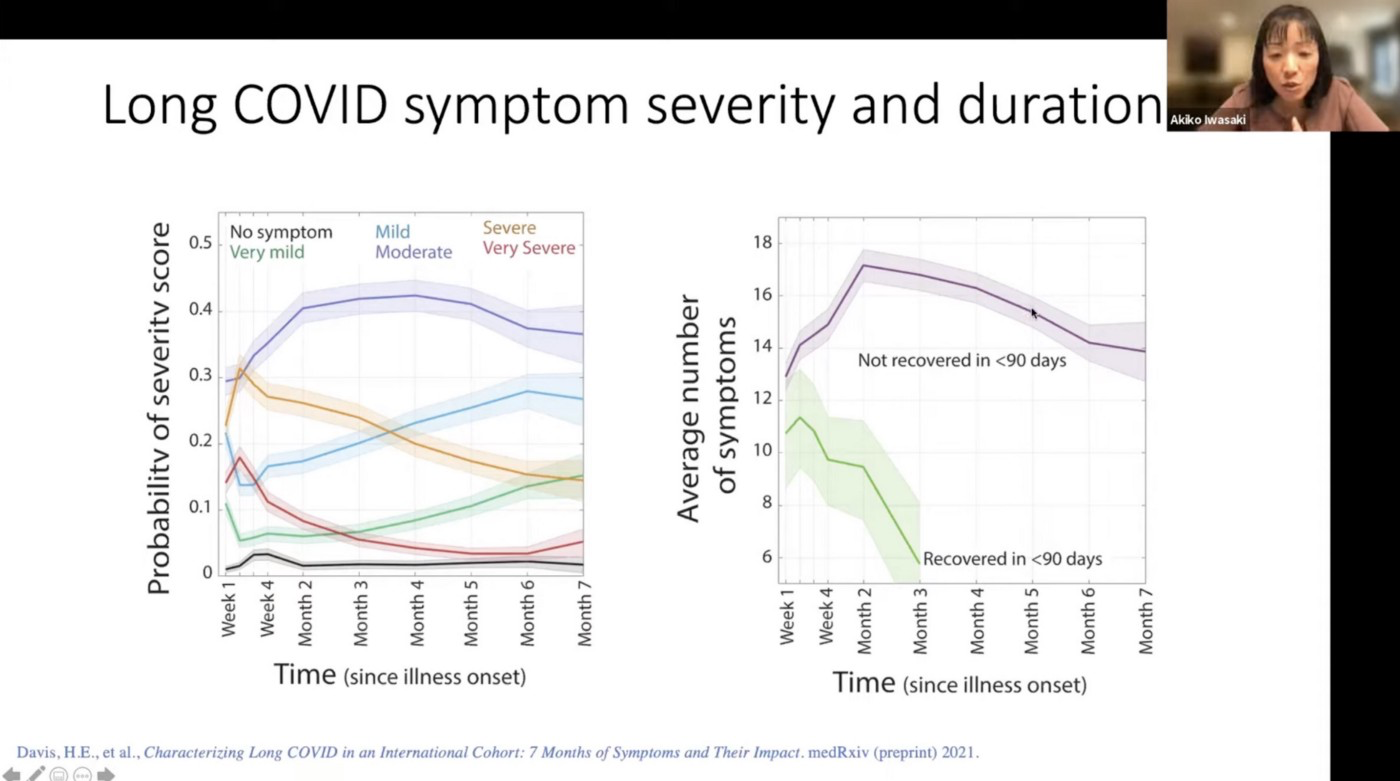
As Iwasaki cites, while the severe symptoms of Long COVID seem to decline, the moderate symptoms go troublingly flat and mild symptoms can increase. Please note that ‘moderate’ and ‘mild’ are scientific terms, not how we use the terms in ordinary life. As survivor Callum O’Dwyer said, his ‘mild’ COVID case has been completely debilitating.
Just a reminder that my case of Covid was assessed to be *mild* and now I can’t live independently, can’t work and must rest before and after a shower. Please please please let’s not lose sight of the risks.
— Callum O'Dwyer (@callumjodwyer) December 5, 2021
Long COVID Can Be Treated
If you’re reading this and you have Long COVID A) I’m sorry and B) I’m not saying your Long COVID can be treated. While we call Long COVID one thing, it’s an array of symptoms, organs, and different people infected with different variants of the virus. Certain treatments do seem to have an impact, but not necessarily for you. That sucks.
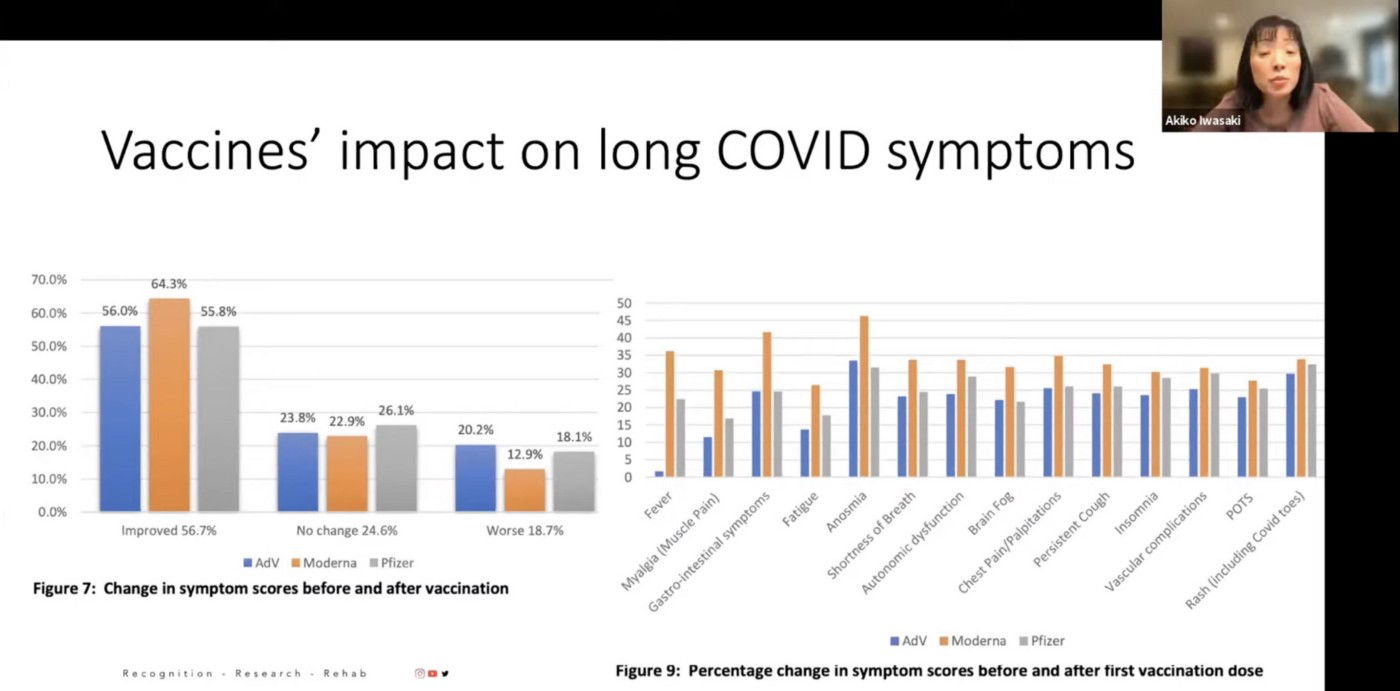
In this survey by the patient group Long COVID SOS (which is not a study), upwards of 60% who got vaccinated (after being sick) reported improvement. Patients have been reporting this effect for a long time and, as Iwasaki said, “The patients are the experts in their disease.”
In a pre-print study, it was demonstrated that “vaccination in Long COVID patients seems to double the rate of complete remission in long-haul symptoms.” The possible mechanism for this is that vaccination would clear ‘viral ghosts’ or that the vaccines could reboot your autoimmune system, at least for a limited time. Unfortunately some people report symptoms coming back again.
Still treatment is what Iwasaki and other researchers are working towards. Right now they’re trying to figure out the molecular basis so they can “target the right pathway in the right patient,” ie, to understand the general phenomenon enough to help you. To that end they have three cohorts of miserable people who will inshallah help us all.
As Iwasaki says, “all of these things are done in collaboration with the patients.” She continued, “We want to involve patients as equal partners in these investigations. I have to say that I’ve learned so much over the last many months from talking to and interacting with patients. Patients are the experts of their disease. The least we can do is provide the data back and involve them in the actual analysis and sharing of the data.”
Ultimate these patients are people, like you or me, that have been sacrificed to some false economic gods, to the idea that we should just ‘live with the virus’. Now they’re literally living with a fucking virus in their bodies and immune systems gone haywire. Now they have to sacrifice even more to unfuck a situation that should have never got so fucked up. We owe them a lot.
As they say, an ounce of prevention is worth a pound of cure, so here we are. Peoples bodies are literally taking a pounding, and don’t know the cure. We don’t even understand the problem yet, but we can confidently say that Long COVID is real, it’s really serious, and that we need to take survivors seriously. Hence the most important part of talking about Long COVID is this. Survivors been talking. We need to fucking listen.
Watch the lecture and follow Dr. Iwasaki on Twitter