The Problem With Public Masking
Most infection happens in private
Wear a mask, but please understand that it’s not enough. In a study of 11,000 infections, only 0.5% happened in public. The vast majority of infection happens where you sleep, work, or eat. Where we don’t wear masks.
That’s the problem. Public masking is vital, and shows that you give a shit, but on its own it’s insufficient. It has to be part of many public health measures, not the only part.
The clusters
Gwenan Knight and her team at the London School of Hygiene and Tropical Medicine went through scientific literature and news reports to see where people were getting infected by COVID-19.
It wasn’t in public.
Households were the most common place for transmission, accounting for 15 percent, or 38 of 231, cluster events. And mealtime was prime time. “It’s not the eating. It’s the sitting around and talking,” Noymer suspects. (Science News)
In their published data, 2% of cluster events were in public and only 0.5% were on transport. And very few people were infected in these events, just 0.55% of the total. We have mandates on public masking, but that seems to be where masking is the least needed*.
But let’s expand the definition of public a bit beyond the street. What about shops, bars, churches; all the places we ‘go out’? I’ve colored them in blue:
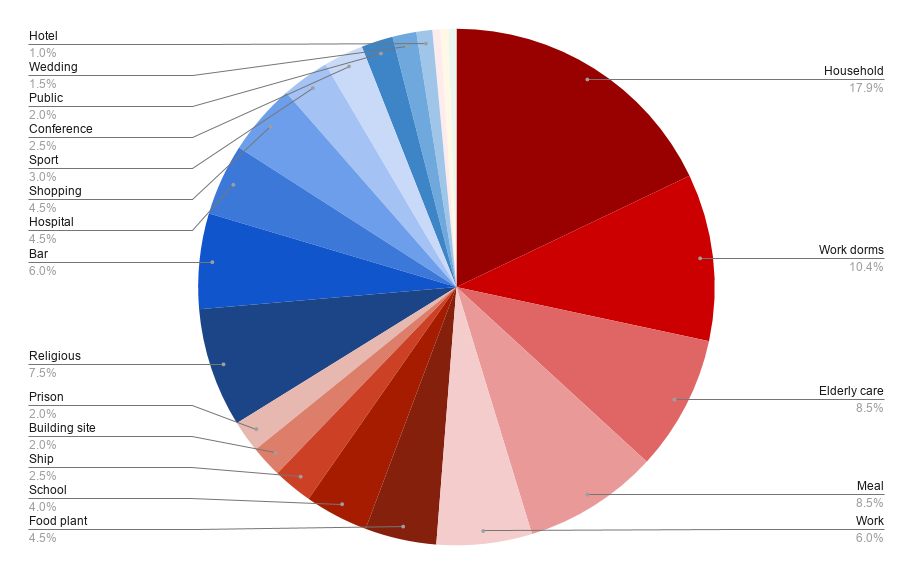
Even with this expanded definition, only ⅓ of clusters** were in public. That’s a lot, and these are events that could connect other clusters. So mask up! But we must still remain aware; 66% of infections are happening (literally) behind closed doors.
But what about Japan?

People say that Japan beat COVID-19 with just masks. This isn’t true. Japan had a very complicated response, of which public masking was just one part.
As Dr. Tomoya Saito (National Institute of Public Health) said, their response included a lot of “time-consuming public health work”. Most obviously, Japan had an existing infrastructure of 25,000 contact tracers over 469 offices. They were also really smart about finding super-spreaders.
While everyone was tracing forwards, to see who you might have infected, Japan was tracing backwards, to find the super-spreader that infected you. This enabled them to quickly lock down clusters, without mass testing. This epidemiological investigation also revealed how exactly the virus spread — through close contact and poor ventilation.
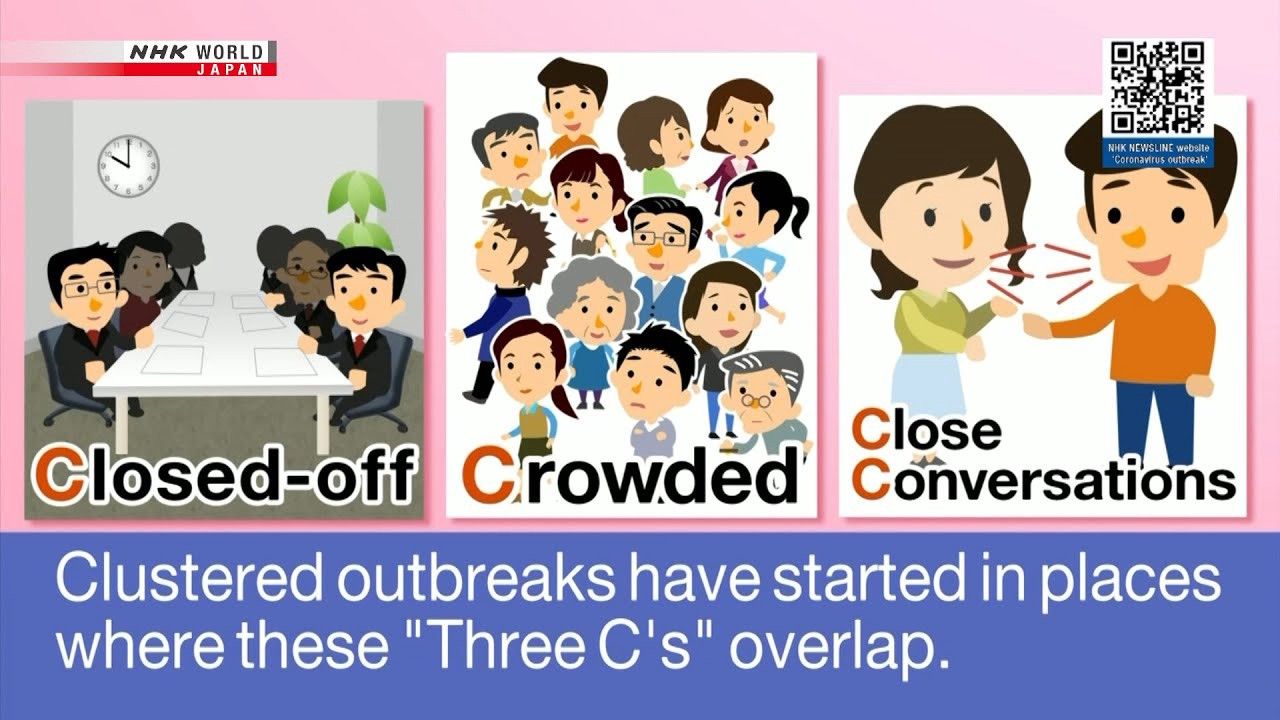
Once they learned these risk factors they quickly communicated it as the Three-Cs (closed, crowded spaces with close contact). Thus the public didn’t just mask and hope for the best, they were aware of the conditions for private transmission and tried to avoid them.
So, no, it wasn’t just masks that saved Japan. That’s like pointing to a battle flag and saying ‘what a great army’. Flags are great, but you also need guns, and troops, and supply lines, and planning.
What about us?
I write this because I’m guilty. Where I live, we have 100% masking in public, and 0% in private. I was recently at a funeral, sitting outdoors and wearing a mask, but then I went into a closed, poorly ventilated room to eat. With my mask off obviously, how else would I access my food-hole? Other people were there, smoking and chatting. That’s exactly how COVID-19 spreads.
I look right, but I’m doing wrong. Because the risk just isn’t where we expect. The call is coming from inside the house.
It’s like child molesters, really. We’re super paranoid about strangers, but most abusers are known — they’re family and friends. That’s how COVID-19 works as well.
We can’t just cover our faces in public and think that keeps our family and friends safe. Our family and friends are the problem.
As Henry Hill says in Goodfellas,
If you’re part of a crew, nobody ever tells you that they’re going to kill you. It doesn’t happen that way. There aren’t any arguments or curses like in the movies. See, your murderers come with smiles. They come as your friends, the people who have cared for you all of your life, and they always seem to come at a time when you’re at your weakest and most in need of their help.
The scary thing is that this is how COVID-19 works as well. It’s not a stranger on the street that infects you, it’s your cousins, or your co-workers, and they come with a smile. Masks alone can’t protect us from this. We can’t and generally won’t wear masks all the time. We need the invisible shield that is public health.
Americans think that just winning the masking debate (why?) will make them safe, but that’s just table stakes. That’s just the battle-flag of public health, not the weaponry, the army, and — most importantly — the strategy. The countries that mask do much more than that, they have sophisticated public health systems — from Ghana to South Korea — and the public support and sacrifice to back them up.
So by all means, wear a mask. It’s both an act and a sign of good public health. Then demand all the invisible public health stuff as well. Remember that public masking covers private sins. The only absolution is all the tools of public health.
Leclerc QJ, Fuller NM, Knight LE et al. What settings have been linked to SARS-CoV-2 transmission clusters? [version 2; peer review: 2 approved]. Wellcome Open Res 2020, 5:83 (https://doi.org/10.12688/wellcomeopenres.15889.2)
*It is possible that cluster rates in public are low because of masking, but the Knight dataset includes a lot from where masking rates were low, like the US, Germany, Australia, etc.
**The study counted clusters (infections with oneish source), but one cluster could have multiple infections. For example, the Diamond Princess cluster was one cluster with over a thousand cases. You can see the full dataset here. You can also see the tables I used here.